
22q11 deletion syndrome
Codes
ICD-10: D82.1
ORPHA: 567
General information
Estimated occurrence
25:100,000 live births.Cause
Chromosomal deletion of a small amount of material on the long arm (q) of chromosome 22. Autosomal dominant heredity. In most cases the 22q11-deletion syndrome is a spontaneous mutation.General symptoms
| C | Cardiac defect, various congenital cardiac malformations |
| A | Abnormal faces, deviant facial features |
| T | Thymic hypoplaisa/aplasia, very small thymus gland or none at all, increased risk of infection |
| C | Cleft palate, most commonly covert (submucous) clefting |
| H | Hypocalcemia, calcium deficiency attributable to poorly functioning or absent parathyroid glands |
| 22 | Deletion of chromosomal material on chromosome 22 |
Other malformations including deformity of the kidneys, clubfoot, hearing and vision problems as well as behavioral aberrations and learning difficulties may occur. There are varying combinations of symptoms, as well as a substantial variation in degree of severity.
Synonyms
CATCH 22, Di George syndrome, Velocardiofacial syndrome.Images
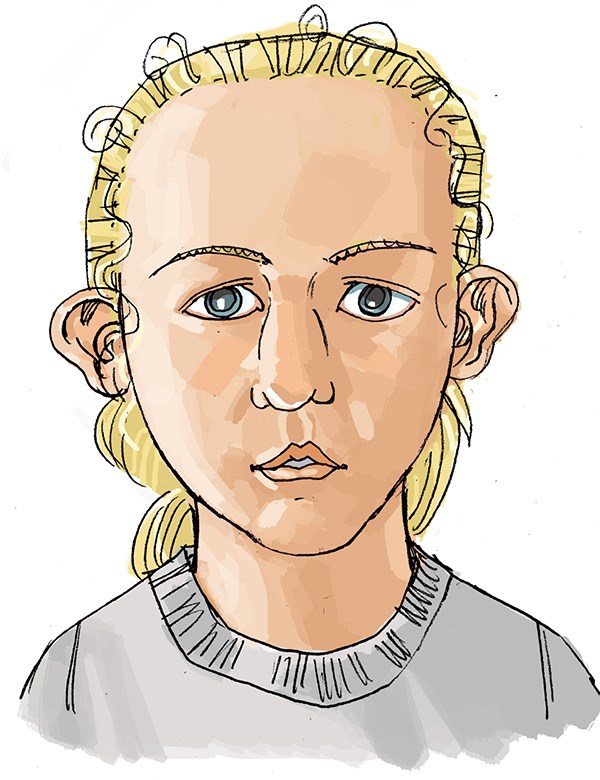
Characteristic facial features in 22q11 deletion syndrome:
Broad nasal bridge. Round tip of the nose. Eyelid hooding. Strabismus. Thin lips. Cup-shaped ears.

Orofacial/odontological symptoms
Certain facial features are characteristic for the diagnosis. Hypernasal speech is a very common problem. Eating disorder may occur. Aberrations in tooth mineralisation taking the form of spotting or pitting of the tooth enamel are common. Deformed teeth, known as peg shaped teeth, and occasional missing tooth buds are more frequent than in healthy individuals. Delayed dental development is also often found. An increased incidence of lingua geografica and a tendency to bleed easily from the oral mucousa have been reported, as well as poor oral hygiene, frequent caries and gingivitis (inflamed gums).Advice on follow-up and treatment
- It is important that individuals with 22q11-deletion syndrome come in early contact with the dental services for extra preventive dental care and information about oral hygiene. Frequent infections, poor nutrition, and poorly mineralized enamel all increase the risk of caries.
- X-ray to determine the presence of tooth buds may be needed around the age of 7 to 9.
- An orthodontist should be consulted between the ages of 7 and 9 in order to identify dental aberrations or malocclusions and to plan any necessary orthodontic treatment.
- In cases of defective palate, a specialist team will be needed for follow up and treatment.
- When treating medically compromised patients always contact their doctors for medical advice (bleeding problems, heart diseases etc).
- Feeding and swallowing difficulties are investigated and treated by a specialist team at the hospital or multidisciplinary treatment center.
Sources
National Board of Health and WelfareUpdated: 2019-11-12 14:19
Please share this page through:





