Spinal muscular atrophy
This is the text from the oral care programme for people with Spinal muscular atrophy (SMA).
Mun-H-Center, a Swedish orofacial resource center for rare diseases and a specialist dental clinic, has gathered knowledge and experience over many years on the clinical care of patients with spinal muscular atrophy (SMA). This document compiles the key insights we have gained regarding the care and treatment of this patient group. People with SMA are often medically fragile. The mouth opening capacity can be reduced and impaired orofacial function can occur. These issues, combined with risks associated with anaesthesia, demand enhanced dental care to prevent oral diseases.
Background
Spinal muscular atrophy is a neuromuscular disease caused by a defect on chromosome 5. SMA types I, II, and III are autosomal recessive inherited conditions. In SMA, the motor neurons in the brainstem, medulla oblongata and spinal cord degenerate, leading to muscle weakness and atrophy – particularly in the chest, back, and neck. Intellectual development is not affected.
SMA I (Werdnig-Hoffmann disease): Symptoms are present from birth or appear before six months of age. Infants with SMA I cannot lift their heads due to weak neck muscles. Breathing function is severely affected, and there is a high risk of infections.
SMA II (so called intermediate form): Symptoms appear between six and 18 months of age. Muscle weakness is usually more pronounced in the legs than in the arms. Scoliosis (curved spine) is common. Breathing function may be affected.
SMA III (Kugelberg-Welander disease): Symptoms appear around two years of age or later. Muscles closest to the torso (proximal muscles) are weakened. Back problems and difficulty walking are common and may worsen over time. Weak throat muscles affect swallowing ability. Tongue muscles may also be weak, showing fasciculations (small twitches). Reduced mouth-opening ability is common among children, adolescents, and adults with SMA. Various types of dental malocclusions
can occur.
Dental care for people with SMA
Need for preventive dental care
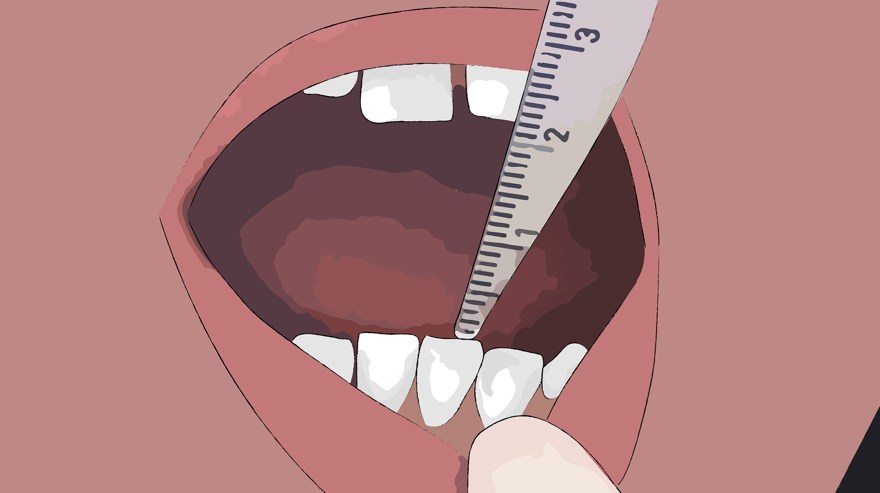
It is important for children to establish early contact with dental care, preferably with a paediatric dentist. Individuals with SMA require regular and enhanced dental care to maintain good oral health. The opening capacity of the mouth should be monitored yearly. All individuals with SMA, regardless of age, need to regularly exercise jaw movements for preventive purposes. If mouth-opening ability decreases, jaw joint function should be investigated and appropriate treatment initiated. If there are difficulties eating through the mouth and the person uses alternative nutrition methods such as gastrostomy, this also necessitates special dental care to maintain oral health and prevent sensitivity or aversion to activities like tooth brushing and dental examinations.
Risk factors for oral health
Reduced mouth-opening ability can make oral and dental care difficult. Therefore, it is important to plan ahead for potential extractions of molars, including wisdom teeth. If oral motor skills are affected, food can remain in the mouth after meals, increasing the risk of cavities and periodontal disease. Reflux and nausea can lead to erosion damage to the teeth.
Guidance for relatives, assistants, and healthcare professionals
Individuals with SMA may need help from relatives, assistants, and healthcare professionals to perform oral care at home. Practical guidance from dental care providers and access to oral care aids are necessary for them to do this properly.
Exercise program for stretching jaw muscles
 |
Time to train your jaw! Exercise program for: |
 |
Open your mouth as wide as you can. |
 |
Push your lower jaw forward. |
 |
Move your jaw to one side... |
 |
...and to the other side. |
 |
Open your mouth wide again. |
 |
Use your hand to stretch... |
 |
...or your Therabite... |
 |
...or Jaw trainer. |
 |
Please feel free to contact us if you have any questions! Best regards, (fill in the practitioner’s name and the clinic’s phone number) |
About the oral care programme
- Authors: Anna Ödman Roussakis, specialist dentist in orthodontics, Annette Carlsson, dental hygienist, Lisa Bengtsson-Stelzer, speech language pathologist, and Åsa Mårtensson, hospital dentist, Mun-H-Center.
- Layout, photos, and cover image: Inga Svensson, previous communicator, Mun-H-Center.
- Illustrations in the exercise program: Komhit.
- Translation: Hanna Samara, communicator, Mun-H-Center
- Print: 2024