Silver-Russell syndrome
Codes
ICD-10: Q87.1G
ORPHA: 813
General information
Estimated occurrence
Very rare.Cause
In approximately 50 percent of individuals with Silver Russell syndrome the cause is unknown. The most common known cause is a defect on chromosome 11 (11p15) but in some individuals a change has been found in chromosome 17 and in others in chromosome 7.
General symptoms
Children with Silver-Russell syndrome are small at birth. These children do not gain weight or grow satisfactorily. The body often develops asymmetrically. The hands and feet tend to be small and the fifth finger, which grows slowly, eventually curves inward. Muscular weakness and delayed motor development are common. Learning disability is found in approximately 30 percent of these children. The average adult length of individuals with the syndrome who do not receive growth hormone treatment is approximately 140 cm (4 feet 7 inches) for women and approximately 150 cm (5 feet) for men.
Synonyms
Russell-Silver syndrome, Silver syndrome.
Images

Orofacial/odontological symptoms
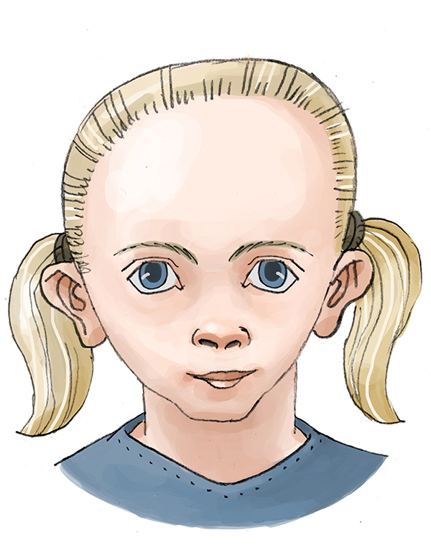
Children with Silver-Russell syndrome often have a special facial shape (triangular shaped face), the face being short and the mouth downwardturned. The head is large in relation to the body. Other characteristics include small jaws, a small, narrow chin, and a narrow, high palate. The occurrence of a large overbite is somewhat more common in these children than in a control group, as well as deep bite. The eruption of permanent teeth is often delayed one year. The teeth may be small and short. Enamel defects on the primary teeth and on the permanent frontal teeth is a frequent finding. Feeding impairment is common in children.
Advice on follow-up and treatment
- Children with eating problems often require supplementary dental care, including help with their oral hygiene and fluoride treatment.
- Regular check-ups of dental and jaw development. Orthodontist should be consulted when needed.
- Feeding and swallowing difficulties are investigated and treated by a specialist team at the hospital or multidisciplinary treatment centre.
- A speech therapist may provide practical advice regarding feeding, as well as instruction for the stimulation of the mouth muscles.