
Gastrostomy
This is the text from the oral care programme for children and adolescents with a gastrostomy.
The dental care teams at Mun-H-Center have many years’ experience of clinical care of children and adolescents with a gastrostomy. This leaflet summarise the most important aspects of meeting and treating this group of patients.
Background
When a child or adolescent has feeding difficulties, and adapted food or dietary supplements cannot meet their nutritional and energy needs, nutrition can be provided by other means than through the mouth. This can be done intravenously – parenteral nutrition – or through the gastrointestinal tract – enteral nutrition. When enteral nutrition is needed for a longer period of time, a feeding tube can be inserted through the abdomen into the stomach – this is known as a gastrostomy. This oral care programme will use the term gastrostomy, even if children and adolescents with severe feeding difficulties can receive feeding support by various means.
Gastrostomy can be used in a broad range of different morbidities. Having a gastrostomy is common in children and adolescents with neurological disorders, as well as in the event of rare medical conditions. Some patients will have a gastrostomy for a limited period while others need nutrition via gastrostomy throughout their lives.
Carrying out oral hygiene procedures on children and adolescents with a gastrostomy can be a challenge. Reduced oral motor control and difficulties handling fluids in the mouth are common. Involuntary bite and vomiting reflexes can occur, which complicate the procedure. Cognitive functional impairment and neuropsychiatric conditions, often in combination with hypersensitivity in the mouth, are also difficulties which occur and which affect treatment as well as the oral hygiene procedure at home.
Many children with a gastrostomy are in contact with multi-professional dysphagia teams, nutrition teams or habilitation. These can be important collaboration partners in caring for children and adolescents with a gastrostomy.
Dental care for children and young people with a gastrostomy
Need for preventive dental care
It is important for children to come into contact with dental care services, ideally a pediatric dentist, at an early stage. Children and adolescents with a gastrostomy need regular and reinforced dental care in order to maintain good oral health.
Risk factors for oral health
Swallowing problems are a common reason for needing nutrition by other means than through the mouth. Swallowing problems imply an increased risk of choking and aspiration, which is important to bear in mind in connection with dental treatment.
Receiving nutrition by other means than through the mouth affects oral health. A person who only eats small amounts, or nothing at all, through their mouth can easily develop hypersensitivity in the mouth, which can lead to difficulties accepting both self-care and treatment by dental care services. If oral motor function is reduced, this leads to a deterioration of self-cleaning and a risk that food remains in the mouth. This in turn implies an increased risk of developing gingivitis, and in some cases caries. These problems are made worse if xerostomia, or dry mouth, also occurs. Calculus forms easily and abundantly when a person’s mouth is inactive. Gastroesophageal reflux and frequent vomiting have an eroding effect on the teeth. Weak orofacial muscles and imbalances between the intraoral and perioral muscles affect the development of the face, jaws and dental arches, which can lead to malocclusion, and this should be monitored regularly.
Guidance for family members and assistants
Children and adolescents with a gastrostomy may need help from dependents and carers to carry out oral hygiene. In order for them to be able to help in the best possible way, they need practical guidance from the dental care services as well as access to oral hygiene aids.
Treat the patient in seated/half-seated position:
- in the event of discomfort lying down due to e g breathing difficulties.
- in the event of reduced ability to cough and swallow.
Work in brief sessions:
- if the child/adolescents needs to change their sitting position
- if the child/adolescents has problems breathing or with mucus formation.
- if the child/adolescents has a reduced general condition and is tired.
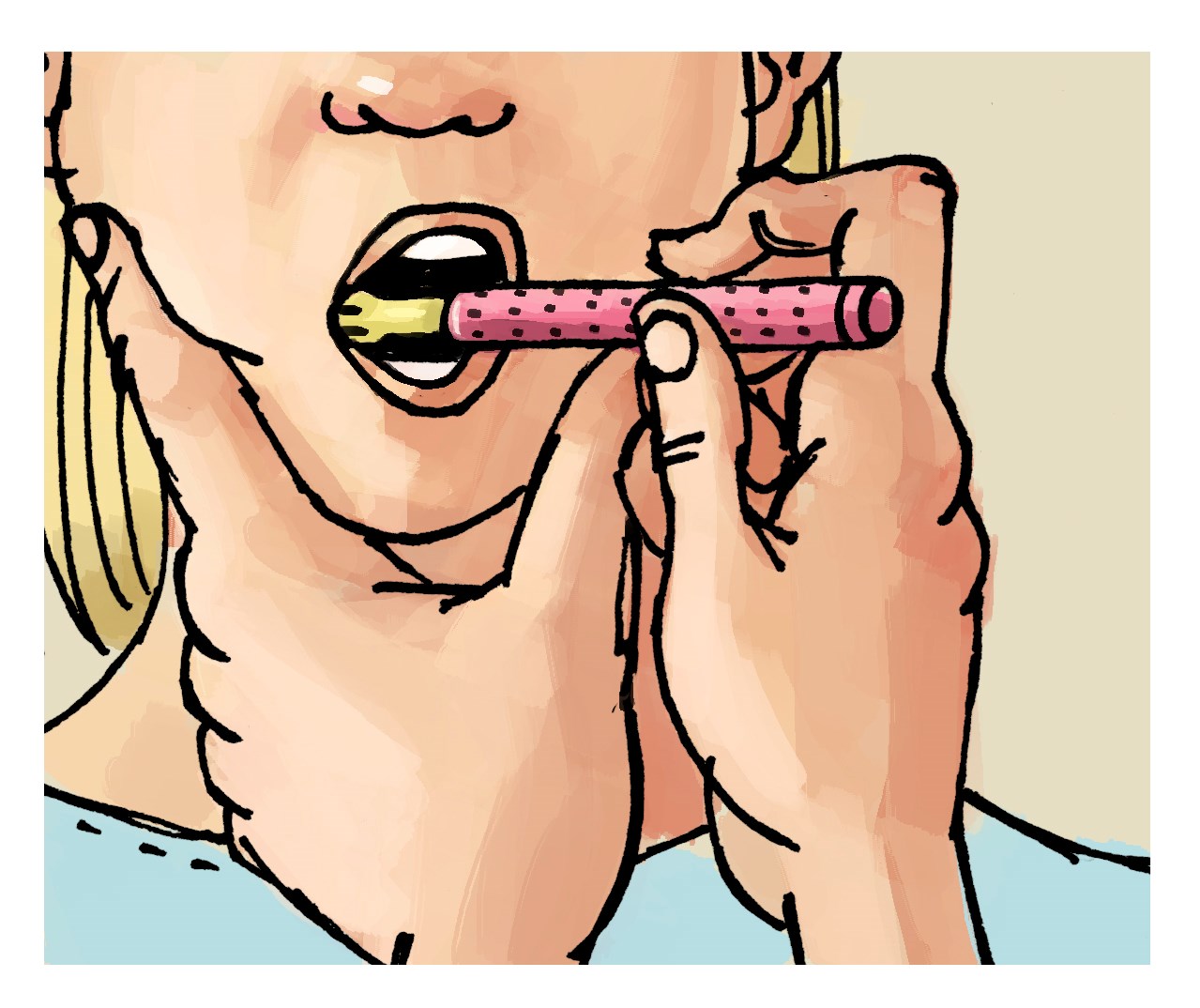
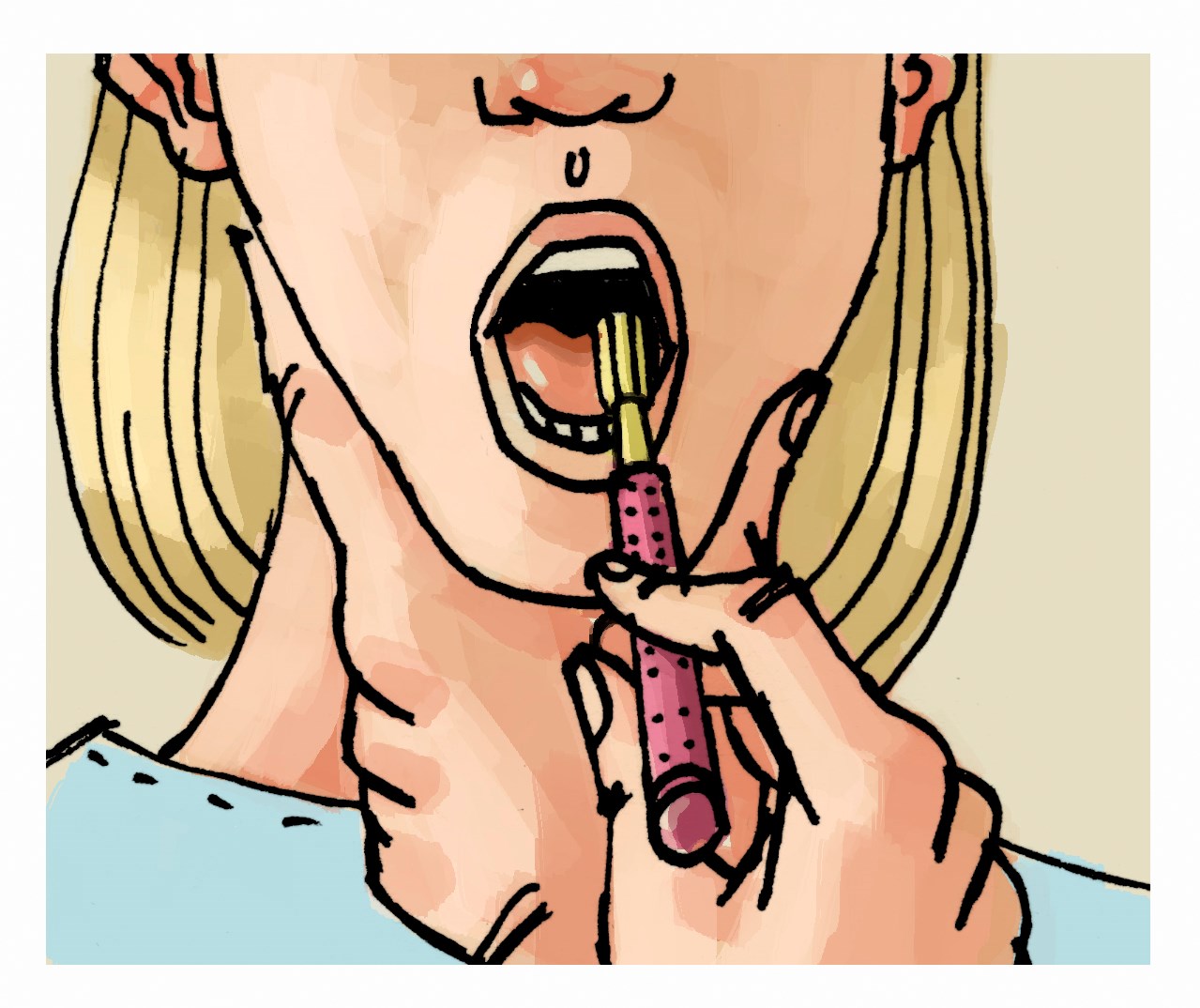
Equipment that should be available to facilitate treatment: bite support, mouth angle expander, oral wipes.
For desensitisation procedures a vibrating appliance, such as a basic electric toothbrush or a Z-vibe oral motor tool, can be useful.

Printed version
If you would like further guidance about dental treatment and oral care for children with a gastrostomy, or if you have any feedback about the oral care programme, please contact us.
About the programme
- Authors: Anna Nielsen Magnéli, Dental Hygienist and Lisa Bengtsson, Speech-Language Pathologist, Mun-H-Center
- Layout and photographs: Inga Svensson, Communicator, Mun-H-Center.
- Printed: 2021
Other languages
- Swedish - change language in the top menu to go to the Swedish website.





